The vasodilating effect of spinal dorsal column stimulation is mediated by sympathetic nerves - Springer: "Immediately after sympathectomy, the contralateral right arm became increasingly cold and cyanotic and the patient complained of chronic painful coldness and severe cold-intolerance in the right arm. Attempts to pharmacologically vasodilate the arm with felodipine did not affect the local vasoconstriction and pain. Dorsal column stimulation (associated with symmetrical paraesthesia in both arms) induced an immediate and marked (ten-fold) increase in skin blood flow in the right arm (and in the leg), whereas skin blood flow in the left arm remained unaffected. The lack of vasomotor response in the left arm was not due to maximal vasodilatation at rest, since skin blood flow in the left arm showed a normal capacity for axon reflex vasodilatation following antidromic activation of sensory afferents. The results suggest that the marked vasodilatation induced by dorsal column stimulation is mediated by sympathetic vasomotor fibres, via modulation of central neuronal circuits involved in the regulation of skin sympathetic discharge."
'via Blog this'
Monday, December 10, 2012
Saturday, December 1, 2012
Transection below T8-T10 is not accompanied by reflex sweating
Reflex sweating in patients with spina... [Arch Phys Med Rehabil. 1977] - PubMed - NCBI: "Sweat glands derive their innervation from the sympathetic nervous system. The spinal sympathetic structures that are located in the intermediolateral areas extend from T1-L2 segments and are under the control of hypothalamic centers. Cord transection abolishes the supraspinal control of sudorimotor function. Since sympathetic innervation does not follow a clear segmental distribution, normal sweating may be preserved at a higher or lower level than skin sensation. Nonthermoregulatory reflex sweating is an indication of unchecked spinal cord facilitation and is precipitated by afferent stimuli from bladder, rectum, and various other sources. It is usually a manifestation of mass reflex or autonomic crisis and occurs particularly in cervical or high thoracic lesions. Transection below T8-T10 is not accompanied by reflex sweating. The phenomenon of thermal relfex sweating is controversial. Although some aspects of nonthermoregulatory reflex sweating are still unclear, proper immediate and continuing preventive management will reduce the incidence of this and other autonomic manifestations. "
'via Blog this'
'via Blog this'
Monday, November 26, 2012
Hemodynamic changes in vertebral and carotid arteries were observed after sympathicotomy for hyperhidrosis
T3 sympathicotomy segment was the most frequent transection done (95.83%), as only ablation (25%) or in association with T4 (62.50%) or with T2 (8.33%). It was observed increase in RI and PI of the common carotid artery (p < 0.05). The DPV of internal carotid artery decreased in both sides (p < 0.05). The SPV and the DPV of the right and left vertebral arteries also increased (p < 0.05). Asymmetric findings were observed so that, arteries of the right side were the most frequently affected.
CONCLUSIONS: Hemodynamic changes in vertebral and carotid arteries were observed after sympathicotomy for PH. SPV was the most often altered parameter, mostly in the right side arteries, meaning significant asymmetric changes in carotid and vertebral vessels. Therefore, the research findings deserve further investigations to observe if they have clinical inferences.
http://www.ncbi.nlm.nih.gov/pubmed/16186983
Thursday, October 25, 2012
Research indicates that a highly variable heart rate increases your capacity to respond and adapt to life’s challenges.
Research has shown that reductions in heart rate variability are a predictor of sudden cardiac death, even in individuals without a prior history of cardiovascular disease.
http://theconversation.edu.au/depression-can-break-your-heart-literally-1102
http://theconversation.edu.au/depression-can-break-your-heart-literally-1102
Monday, October 22, 2012
Unexpected beneficial effect of stellate ganglion block in a schizophrenic patient
Unexpected beneficial effect of stella... [Can J Anaesth. 2002 Aug-Sep] - PubMed - NCBI: "Unexpected beneficial effect of stellate ganglion block in a schizophrenic patient"
Stellate ganglion block may relieve hot flashes by interrupting the sympathetic nervous system
Stellate ganglion block may relieve hot flash... [Med Hypotheses. 2007] - PubMed - NCBI: "the wide range of conditions that have been reported to respond favorably to stellate ganglion block suggest that its effectiveness may not be solely the result of increased blood flow nor restricted just to its sphere of innervation. We have found that stellate ganglion block is effective in the treatment of hot flashes in postmenopausal women, as well as those with estrogen depletion resulting from breast cancer treatment. Based on evidence that hot flashes may be centrally mediated and that the stellate ganglion has links with the central nervous system nuclei that modulate body temperature, we hypothesize that the stellate ganglion block provides relief of hot flashes by interrupting the central nervous system connections with the sympathetic nervous system, allowing the body's temperature-regulating mechanisms to reset. If this mechanism can be confirmed, this would provide women with intractable hot flashes with an effective, potentially long-lasting means of relieving their symptoms, and potentially widen the range of indications for stellate ganglion block to include other centrally mediated syndromes."
'via Blog this'
'via Blog this'
Thursday, October 18, 2012
These observations further emphasize our ignorance of the mechanisms responsible for primary hyperhidrosis and of the effect of sympathetic ablation
"These observations further emphasize our ignorance of the mechanisms responsible for primary hyperhidrosis and of the effect of sympathetic ablation on the function of the remaining sympathetic system."
"Only investigators who deviate from accepted standards innovate and thus advance science. Obviously, such deviations may also result in disasters;"
Statement made by the former President of the International Society of Sympathetic Surgery, and ETS surgeon, Moshe Hashmonai (Invited Commentary) Endoscopic Lumbar Sympathectomy Following Thoracic Sympathectomy in Patients with Palmoplantar Hyperhidrosis
World J Surg (2011) 35:54–55 DOI 10.1007/s00268-010-0809-5
Monday, September 24, 2012
Post-sympathectomy pain
Postsympathectomy limb pain, postsympathectomy parotid pain, and Raeder's paratrigeminal syndrome are pain states associated with the loss of sympathetic fibres and in particular with postganglionic sympathetic lesions. There is a characteristic interval of about 10 days between surgical sympathectomy and onset of pain. It is proposed that this pain in man is correlated with the delayed rise in sensory neuropeptides seen in rodents after sympathectomy. These chemical changes probably reflect the sprouting of sensory fibres and may result from the greater availability of nerve growth factor after sympathectomy. The balance between the sensory and sympathetic innervations of a peripheral organ may be determined by competition for a limited supply of nerve growth factor.
Lancet. 1985 Nov 23;2(8465):1158-60
http://www.ncbi.nlm.nih.gov/pubmed/2414615?dopt=Abstract
Lancet. 1985 Nov 23;2(8465):1158-60
http://www.ncbi.nlm.nih.gov/pubmed/2414615?dopt=Abstract
A significant admission from an ETS surgeon, President of the ISSS:
"General represents the ESB (whether as ETS as ETSC or ELS) a substantial interference in regulatory processes of the body represent the decision for this operation requires that previously conservative treatments were made. An ESB is therefore at the end of a treatment history, and never at the beginning."
http://www.dhhz.de/index....;subPage=§ion=32
it is an automatic translation (google) from german, so you have to look at what the 'gist' of what he is saying: ETS, ESB = "a substantial interference in regulatory processes of the body"
Friday, August 31, 2012
Sympathectomy to treat the urge to smoke
Lipov, Eugene (Chicago, IL, US) treating addiction with disruption of the sympathetic chain.
Wednesday, August 15, 2012
"sympathectomy highlighted the disparity between what is known in practice and what appears in the literature"
The March 2004 edition was quite outstanding, with an excellent editorial reminding the reader that only good results are published. The review on thoracoscopic sympathectomy highlighted the disparity between what is known in practice and what appears in the literature.
‘Know Your Results’, the topic of the ASGBI Annual Scientific Meeting, is of outstanding importance; what is more, the surgeon has to go on knowing his/her results to ensure standards of practice do not slip.
The Journal appreciates comments and criticism and the correspondence column remains a crucial part of the BJS in its interaction between editors and reader. It is also part of the scientific process.
A more robust and incisive criticism of articles known to be flawed would prevent the retractions that have recently been published in the Lancet.
Christopher Russell, Chairman, BJS Society
Association of Surgeons of Great Britain and Ireland, ANNUAL REPORT 2004
Monday, August 13, 2012
sympathectomy induced morphological alterations in the masseter muscles
Sympathectomized animals showed varying degrees of metabolic and morphological alterations, especially 18 months after sympathectomy. The first five groups showed a higher frequency of type I fibres, whilst the oldest group showed a higher frequency of type IIb fibres. In the oldest group, a significant variation in fibre diameter was observed. Many fibres showed small diameter, atrophy, hypertrophy, splitting, and necrosis. Areas with fibrosis were observed. Thus cervical sympathectomy induced morphological alterations in the masseter muscles. These alterations were, in part, similar to both denervation and myopathy. These findings indicate that sympathetic innervation contributes to the maintenance of the morphological and metabolic features of masseter muscle fibres.
Sunday, August 12, 2012
Bilateral cervical sympathectomies should be avoided because of the destruction of cardioaccelerator tone
http://www.hiesiger.com/physicians/physicianrfl.html
SURGICAL SYMPATHECTOMY ON THE SENSITIVITY TO EPINEPHRINE OF THE BLOOD VESSELS OF MUSCULAR SEGMENTS OF THE LIMBS
Pursuing this study of the effect of epinephrine on muscle blood flow, Duff and Swan (10) reported that during intravenous epinephrine infusions the initial marked dilatation was succeeded by a second phase of moderate dilatation in normal but not in sympathectomized limbs. Because of its absence in chronically sympathectomized limbs this secondary vasodilatation was at that time thought to be an indirect vasomotor effect mediated by the sympathetic nerves. Re-examination of their data in the light of some subsequent critical experiments now reveals that the difference which they found between normal and sympathectomized limbs may be ascribed largely to vascular hypersensitivity in the later.
In the present paper these additional data are reported, and are incorporated with those of Duff and Swan(10); the whole material being interpreted to provide evidence that hypersensitivity of the vessels of skeletal muscle in the upper and lower limbs may result from pre- and postganglionic sympathectomy in man.
EFFECT OF SURGICAL SYMPATHECTOMY ON THE SENSITIVITY TO EPINEPHRINE OF THE BLOOD VESSELS OF MUSCULAR SEGMENTS OF THE LIMBS, ROBERT S. DUFF
J Clin Invest. 1953 September; 32(9): 851–857.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC438413/
Wednesday, August 1, 2012
Sympathetic nerves protect against blood-brain barrier disruption
http://www.ncbi.nlm.nih.gov/pubmed/7064183
Monday, June 25, 2012
 http://www.sympatix.fi/blog/?lang=en_
http://www.sympatix.fi/blog/?lang=en_Tuesday, June 12, 2012
Effects of lumbar sympathectomy: abolition of ejaculation, causalgia in 41, general morbidity of 0.6% and mortality rate of 0.6 %, arrhythmias, cardiac decompensation
Goldstein, reviewing the complications of 791 patients undergoing open lumbar sympathectomy reports 10% of specific complications, such as abolition of ejaculation in 22 patients and causalgia in 41, general morbidity of 0.6% (TEP and bleeding) and mortality rate of 0.6 % (arrhythmias, cardiac decompensation or bleeding) 15.
SIMPACTECTOMIA RETROPERITONEOSCÓPICA FOR TREATMENT OF LUMBAR plantar hyperhidrosis RETROPERITONEOSCOPIC lumbar sympathectomy FOR THE TREATMENT OF PLANT HYPERIDROSIS
Marcelo de Paula Loureiro, TCBC-PR ¹, ² Neomar Roman, Sheila Cristina Weigmann ³;
Aline ³ Fontana, Paulo Cesar Bufara Boscardim4
(Rev Bras ECR. Cir. 2007, 34 (4): 222-224).
(translated by google)
SIMPACTECTOMIA RETROPERITONEOSCÓPICA FOR TREATMENT OF LUMBAR plantar hyperhidrosis RETROPERITONEOSCOPIC lumbar sympathectomy FOR THE TREATMENT OF PLANT HYPERIDROSIS
Marcelo de Paula Loureiro, TCBC-PR ¹, ² Neomar Roman, Sheila Cristina Weigmann ³;
Aline ³ Fontana, Paulo Cesar Bufara Boscardim4
(Rev Bras ECR. Cir. 2007, 34 (4): 222-224).
(translated by google)
dynamic cerebral autoregulation is altered by ganglion blockade
We measured arterial pressure and cerebral blood flow (CBF) velocity in 12 healthy subjects (aged 29+/-6 years) before and after ganglion blockade with trimethaphan. CBF velocity was measured in the middle cerebral artery using transcranial Doppler. The magnitude of spontaneous changes in mean blood pressure and CBF velocity were quantified by spectral analysis. The transfer function gain, phase, and coherence between these variables were estimated to quantify dynamic cerebral autoregulation. After ganglion blockade, systolic and pulse pressure decreased significantly by 13% and 26%, respectively. CBF velocity decreased by 6% (P <0.05). In the very low frequency range (0.02 to 0.07 Hz), mean blood pressure variability decreased significantly (by 82%), while CBF velocity variability persisted. Thus, transfer function gain increased by 81%. In addition, the phase lead of CBF velocity to arterial pressure diminished. These changes in transfer function gain and phase persisted despite restoration of arterial pressure by infusion of phenylephrine and normalization of mean blood pressure variability by oscillatory lower body negative pressure.
Conclusions-: These data suggest that dynamic cerebral autoregulation is altered by ganglion blockade. We speculate that autonomic neural control of the cerebral circulation is tonically active and likely plays a significant role in the regulation of beat-to-beat CBF in humans.
Circulation. 106(14):1814-1820, October 1, 2002.
http://www.problemsinanes.com/pt/re/dyslipidaemia/abstract.00003017-200210010-00017.htm;jsessionid=PX6phQHYFG5PD1p2DMS1cJLvG1TbtLLLH0bfJT6vKJgLLx1zn0Xf!1816077220!181195629!8091!-1?nav=reference
Conclusions-: These data suggest that dynamic cerebral autoregulation is altered by ganglion blockade. We speculate that autonomic neural control of the cerebral circulation is tonically active and likely plays a significant role in the regulation of beat-to-beat CBF in humans.
Circulation. 106(14):1814-1820, October 1, 2002.
http://www.problemsinanes.com/pt/re/dyslipidaemia/abstract.00003017-200210010-00017.htm;jsessionid=PX6phQHYFG5PD1p2DMS1cJLvG1TbtLLLH0bfJT6vKJgLLx1zn0Xf!1816077220!181195629!8091!-1?nav=reference
Wednesday, June 6, 2012
Sympathectomy involves division of adrenergic, cholinergic and sensory fibers which elaborate adrenergic substances during the process of regulating viscera
http://pharmrev.aspetjournals.org/content/18/1/611.full.pdf+html
Tuesday, June 5, 2012
effect of bilateral cervical sympathetic ganglionectomy on the architecture of pial arteries
The influence of the cranial sympathetic nerves on the architecture of pial arteries in normo- and hypertension was examined. For this purpose the effect of bilateral superior cervical ganglionectomy was evaluated in normotensive rats (WKY) and stroke-prone spontaneously hypertensive rats (SHRSP). The operations were performed at the age of 1 wk, which is just prior to the onset of ganglionic transmission. The length of the inner media contour was measured and the media cross-sectional area was determined planimetrically, with computerized digitalization of projected photographic images of transversely sectioned pial arteries. Four wk after sympathectomy there was a 20% reduction in media cross-sectional area and a consequent reduction in the ratio between media area and calculated luminal radius in the major pial arteries at the base of the brain in WKY but not in SHRSP. Conversely, in small pial arteries linear regression analysis showed that in WKY subjected to ganglionectomy the relationship between media cross-sectional area and luminal radius was significantly larger in arteries with a radius less than 21 microns compared to untreated WKY. No such effect was seen in the corresponding SHRSP vessels. In addition, the cross-sectional area of the internal elastic membrane (IEM) in the basilar arteries of WKY was measured by means of a computerized image-analysing system. Mean cross-sectional area of the IEM was approximately 45% larger following SE than in control animals. The present findings propose a 'trophic' role for the sympathetic perivascular nerves in large pial arteries of the rat. The increased media-radius ratio in the small pial arteries of the WKY following sympathectomy might reflect a compensatory hypertrophy due to reduced protection from the larger arteries against the pressure load. The inability to detect any morphometrically measurable effect of the sympathectomy in the cerebral arteries of SHRSP is probably explained by a marked growth-stimulating effect of the high pressure load in these animals.
http://www.ncbi.nlm.nih.gov/pubmed/7701941
http://www.ncbi.nlm.nih.gov/pubmed/7701941
Tuesday, May 29, 2012
significant fall in left circumflex coronary flow was proportional to the decline in external heart work due to sympathectomy
http://www.springerlink.com/content/k2n6j4555g16x773/
sympathectomy affects the heart, sweating, and circulation
heart rate was significantly reduced at rest (14%), at sub-maximal exercise (12.3%), and at peak exercise (5.7%), together with a significant increase in oxygen pulse (11.8, 12.7, and 7.8%, respectively). The rate pressure product (RPP) was also significantly reduced following the surgical procedure at all three study stages, while all other physiological variables measured remained unchanged. It is suggested that thoracic-sympathetic denervation affects the heart, sweating, and circulation of the respective denervated region
Eur J Appl Physiol. 2008 Sep;104(1):79-86. Epub 2008 Jun 10.
Eur J Appl Physiol. 2008 Sep;104(1):79-86. Epub 2008 Jun 10.
Sunday, May 20, 2012
Drug warning - Karvezide, AVAPRO HCT - 'you must tell your doctor if you have had sympathectomy'
Tell your doctor if:
* you have had a sympathectomy
* you have been taking diuretics
*you have a history of allergy or asthma
www.racgp.org.au/cmi/swckarvz.pdf

* you have had a sympathectomy
* you have been taking diuretics
*you have a history of allergy or asthma
www.racgp.org.au/cmi/swckarvz.pdf
2. Before you start to take AVAPRO HCT
Tell your doctor if:- you suffer from any medical conditions especially-
- kidney problems, or have had a kidney transplant or dialysis
- heart problems
- liver problems, or have had liver problems in the past
- diabetes
- gout or have had gout in the past
- lupus erythematosus
- high or low levels of potassium or sodium or other electrolytes in your blood
- primary aldosteronism - you are strictly restricting your salt intake
- you are lactose intolerant or have had any allergies to any other medicine or any other substances, such as foods, preservatives or dyes.
- have had a sympathectomy
- you have been taking diuretics
- you have a history of allergy or asthma
Published by MIMS/myDr March 2011
UBM Medica Australia uses its best endeavours to ensure that at the time of publishing, as indicated on the publishing date for each resource (e.g. Published by MIMS/myDr January 2007), the CMI provided was complete to the best of UBM Medica Australia's knowledge.
Thursday, May 17, 2012
Use of stellate ganglion block for the treatment of psychiatric and behavioral disorders
The present invention is directed to a method for the treatment of a patient suffering from psychiatric and behavioral disorders, including post partum depression, post traumatic stress disorder, compulsive smoking, attention deficit hyperactivity disorder, gambling addiction, comprising the step of administering a stellate ganglion block to the patient to alleviate the symptoms. The stellate ganglion block may be followed by a sympathectomy to provide permanent relief.
http://www.freepatentsonline.com/y2007/0135871.html
Kind Code: A1
Saturday, May 5, 2012
nerves that sent blood-pressure-raising flight-or-fight signals to the brain were cut
page 187:
It was a grueling operation called sympathectomy, in which the nerves that sent blood-pressure-raising flight-or-fight signals to the brain were cut...The nerve cutting scrambled signals to her circulatory system. She was cold on one side of her body and warm on the other.
It was a grueling operation called sympathectomy, in which the nerves that sent blood-pressure-raising flight-or-fight signals to the brain were cut...The nerve cutting scrambled signals to her circulatory system. She was cold on one side of her body and warm on the other.
The Happy Bottom Riding Club: The Life and Times of Pancho Barnes (Paperback)
by Lauren Kessler (Author)Wednesday, April 25, 2012
Sympathectomy increased the pain threshold and made the sympathectomized rats hypesthetic
Normal adult rats were sympathectomized at L2-L3. The threshold for thermal noxious pain by hot-plate analgesia test and changes in neuropeptides in the lumbar dura mater and dorsal root ganglia using light microscopic immunohistochemistry were assessed and compared with control rats.
Results: In the hot-plate analgesia test, sympathectomized rats increased their hot-plate latency time compared with that of sham-operated rats. Density of calcitonin gene-related peptide immunoreactive fibers in sympathectomy side of the lumbar dura mater decreased to 45.5% compared with the contralateral side. The number and size of calcitonin gene-related peptide immunoreactive cells in dorsal root ganglia showed no difference between sympathectomized and contralateral side.
Conclusion: Sympathectomy increased the pain threshold and made the sympathectomized rats hypesthetic. A large numbers of sensory fibers innervated the lumbar dura mater via L2-L3 sympathetic nerve in rats. Sympathectomy reduced the number of these nerve fibers in the lumbar dura mater. Sympathetic nerves may play an important role for low back pain involving the lumbar dura mater.
http://journals.lww.com/spinejournal/Abstract/1996/04150/An_Anatomic_Study_of_Neuropeptide.4.aspx
Long-term sympathectomy induces sensory and parasympathetic fibres sprouting, and mast cell activation in the rat dura mater
http://discovery.ucl.ac.uk/1330488/
There are similarities between the delayed onset of the human pain state and the delayed rise in sensory peptides after sympathectomy
The effect of sympathectomy on the calcitonin gene-related peptide (CGRP) level in the rat primary trigeminal sensory neurone was investigated. Six weeks after bilateral removal of the superior cervical ganglion there was a 70% rise in the CGRP content of the iris and the pial arteries, a 34% rise in the concentration in the trigeminal ganglion but no change in the brainstem. The CGRP rise in both end organs suggests that this phenomenon may be common to all peripheral organs receiving combined sensory and sympathetic innervations. The lack of any rise in the brainstem CGRP content raises the possibility that this process spares central terminations. In contrast, the level of neuropeptide Y, a peptide mainly contained in sympathetic terminals, fell to 35% of control values in the iris and pial arteries whilst the trigeminal ganglion and brainstem concentrations remained unchanged. The possible relevance of these observations to the clinical syndrome of postsympathectomy pain (sympathalgia) is discussed. There are similarities between the delayed onset of the human pain state and the delayed rise in sensory peptides after sympathectomy.
http://www.ncbi.nlm.nih.gov/pubmed/3877546
http://www.ncbi.nlm.nih.gov/pubmed/3877546
sympathectomy resulted in complete disappearance of histochemically detected adrenergic and a considerable decrease of cholinergic nerve fibers in the pial arterial walls
sympathectomy resulted in complete disappearance of histochemically detected adrenergic and a considerable decrease of cholinergic nerve fibers in the pial arterial walls. The vasodilatation was much less obvious in sympathectomized than in control animals. This was associated with (and probably caused by) a considerable rise in histochemically detected serotonin activity of the pial arteries walls. After recovery of blood supply to the brain the constriction of the pial arterial active segments restricting the excessive cerebral blood flow, was significantly reduced due, probably, to the sympathetic deprivation. Therefore, the sympathetic control plays an important part in pial arterial responses regulating the adequate blood supply of the cerebral cortex.
http://www.ncbi.nlm.nih.gov/pubmed/7173422
http://www.ncbi.nlm.nih.gov/pubmed/7173422
Monday, April 23, 2012
Digital infrared thermal image after T2 sympathicotomy or T3 ramicotomy.
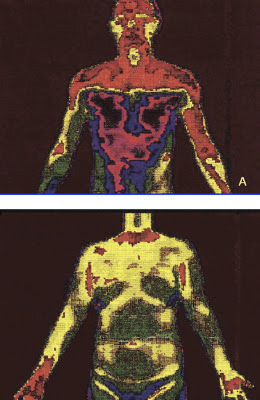
(A) Clear cut change of skin temperature after a T2 sympathicotomy. (B) An even distribution of skin temperature after ramicotomy.
Gossot and colleagues [8] analyzed a group of T2, T3, T4 sympathectomy patients in comparison with a group of patients undergoing a T2, T3, T4 ramicotomy and they reported no statistical difference regarding the incidence of CS between the two groups studied (72.2% and 70.9%). However in terms of the severity of CS (embarrassing, disabling) causing inconveniences to daily life, they reported 27% and 13% incidences in these two groups, respectively. These findings suggest that by preserving the sympathetic trunk, it was possible to reduce the severity of CS.
The preganglionic fibers of the sympathetic nerve to the arm originate mostly from the spinal segments T3–T6 and the postganglionic fibers of the sympathetic nerve to the arm originate from T2 and, to a lesser extent, the T3 ganglia [9]. This implies that the division of preganglionic fibers (rami communicantes) reduces the extent of denervation of the sympathetic nerve as compared with the division of postganglionic fibers (sympathetic trunk) in the treatment of palmar hyperhidrosis. Sympathectomy or sympathicotomy is one of the procedures used to divide the sympathetic trunk. Sympathicotomy distinctively changes sympathetic nerve distribution in comparison with a ramicotomy. Figure 4A illustrates the clear-cut changes of skin temperature after a T2 sympathicotomy. However the overall sympathetic nerve distribution to the body is not markedly changed after a T3 ramicotomy because a T3 ramicotomy is a procedure that is used to divide one of the preganglionic fibers and to preserve the sympathetic trunk. Figure 4B illustrates an even distribution of skin temperature after T3 ramicotomy.
http://ats.ctsnetjournals.org/cgi/content/full/78/3/1052#FIG4
Tuesday, April 10, 2012
most surgeons do not have a clear understanding of their short-term outcomes for the majority of procedures they perform
The public would probably be surprised to know that most surgeons do not have a clear understanding of their short-term outcomes for the majority of procedures they perform.
Of even greater concern is the lack of data on long-term outcomes associated with surgical interventions.
Many surgeons argue that they are too busy and do not have the time and resources to conduct this sort of follow-up. This is not entirely without foundation, but it does seem difficult to defend a stance that says “I will continue to work feverishly at the operations I do but not assess how successful my results are”.
Of even greater concern is the lack of data on long-term outcomes associated with surgical interventions.
Many surgeons argue that they are too busy and do not have the time and resources to conduct this sort of follow-up. This is not entirely without foundation, but it does seem difficult to defend a stance that says “I will continue to work feverishly at the operations I do but not assess how successful my results are”.
Guy Maddern (ASERNIP-s): No excuse for poor surgical outcomes
MJA INSIGHT, 8 August 2011
Monday, March 12, 2012
It’s not unusual to hear people who have undergone sympathectomies describe themselves as feeling emotionally “colder” than before
It’s not unusual to hear people who have undergone sympathectomies describe themselves as feeling emotionally “colder” than before. Among psychologists and neurologists alike there is concern, but no evidence, that the procedure limits alertness and arousal as well as fear, and might affect memory, empathy and mental performance. Professor Ronald Rapee, the director of the Centre of Emotional Health at Sydney’s Macquarie University, says he’s counselled several people who complain of feeling “robot-like” in the long-term wake of the operation. “They’re happy they no longer blush, but they miss the highs and lows they used to feel.”
(John van Tiggelen, Good Weekend Magazine, The Age and the Sydney Morning Herald, 10th March 2012)
(John van Tiggelen, Good Weekend Magazine, The Age and the Sydney Morning Herald, 10th March 2012)
Friday, February 24, 2012
impairment of the CBF autoregulation after unilateral cervical sympathectomy
Although these findings argued against a neurogenic mechanism, James at al. (1969) reported impairment of autoregulation after unilateral cervical sympathectomy in the babbon. Gotoh et al. (1971/1972) observed impairment of autoregulation in patients with the Shy-Drager syndrome.
It was concluded that the autonomic nervous system plays an important role in the mechanism of autoregulation of CBF and that his mechanism is independent of the chemical control of the cerebral vessels. This was confirmed by direct observation of the pial vessels in cats, where separate sites of action in the vascular tree for autoregulation and chemical control were demonstrated; the autoregulatory reaction was located in pial arteries with a diameter larger than 50 μ, and the reaction to carbon dioxide in pial arteries of smaller diameter (Gotoh et al. 1975).
They concluded that the arteries operating in autoregulation were the larger ones with the dense innervation, while the smaller arteries with sparse innervation were involved in chemical control.
Coronna and Plum (1973) demonstrated the absence of CBF autoregulation in a patient with a Shy-Drager syndrome who had a postganglionic denervation.
It was concluded that the autonomic nervous system plays an important role in the mechanism of autoregulation of CBF and that his mechanism is independent of the chemical control of the cerebral vessels. This was confirmed by direct observation of the pial vessels in cats, where separate sites of action in the vascular tree for autoregulation and chemical control were demonstrated; the autoregulatory reaction was located in pial arteries with a diameter larger than 50 μ, and the reaction to carbon dioxide in pial arteries of smaller diameter (Gotoh et al. 1975).
They concluded that the arteries operating in autoregulation were the larger ones with the dense innervation, while the smaller arteries with sparse innervation were involved in chemical control.
Coronna and Plum (1973) demonstrated the absence of CBF autoregulation in a patient with a Shy-Drager syndrome who had a postganglionic denervation.
Gotoh et al (1979) subsequently showed that autoregulation in patients with this syndrome was impaired irrespective of the localization of the damage to the cervical sympathetic nervous system (preganglionic, central, postganglionic) as judged by the eye instillation test.
Handbook of Clinical Neurology,
Vascular Diseases, Part I by P. J. Vinken, G. W. Bruyn, H. L. Klawans, and J. F. Toole
Friday, February 17, 2012
reduced oxygen saturation and shallow respiration after a thoracoscopic sympathectomy
- D. J. Canty1,2,3,* and C. F. Royse4,5
1Department of Anaesthesia, Royal Hobart Hospital, 48 Liverpool Street, Hobart, Tasmania 7000, Australia
- 2Medical School of The University of Tasmania, Tasmania, Australia
- 3Department of Pharmacology, The University of Melbourne, Melbourne, Australia
- 4Anaesthesia and Pain Management Unit, Department of Pharmacology, University of Melbourne, Melbourne, Australia
- 5Royal Melbourne Hospital, Victoria, Australia
- *Corresponding author. E-mail: david.canty@dhhs.tas.gov.au
- http://bja.oxfordjournals.org/content/103/3/352.full
CAUSES AND MANAGEMENT OF ORTHODEOXIA - The Australian Short Course on Intensive Care Medicine, 2005
DEFINE AND LIST THE CAUSES AND MANAGEMENT OF PLATYPNOEA AND
ORTHODEOXIA
p. 79:
Autonomic
o Parkinson disease (Hussain 2004)
o Bilateral thoracic sympathectomy (van Heerdon 2004)
Published in 2005 by
The Australasian Academy of Critical Care Medicine
“Ulimaroa”
630 St Kilda Rd, Melbourne,
Victoria 3004
ISSN 1327-4759
ORTHODEOXIA
p. 79:
Autonomic
o Parkinson disease (Hussain 2004)
o Bilateral thoracic sympathectomy (van Heerdon 2004)
Published in 2005 by
The Australasian Academy of Critical Care Medicine
“Ulimaroa”
630 St Kilda Rd, Melbourne,
Victoria 3004
ISSN 1327-4759
HAZARDS ASSOCIATED WITH CERVICO-THORACIC SYMPATHECTOMY
The following is a case report of a healthy 18-year-old woman who had bilateral Cervico- Thoracic sympathectomy done in two stages for severe hyperhidrosis in the palms of her hands.
Two episodes of asystolic arrest occurred during the 2nd stage left Cervico-Thoracic sympathec- tomy.
Thirty-five minutes after starting the operation, as the surgeon was retracting and dissecting the upper thoracic chain,
the cardiac monitor showed sudden onset of sinus bradycardia. The pulse rate was 50 beats per minute. Atropine 1·2 mg was given intravenously but cardiac asystole occurred.
External cardiac compression was started and another dose of atropine 1· 2 mg was given, followed by adrenaline 1·0 mg but there was no response. Following a second dose of adrenaline 1·0 mg and sodium bicarbonate 100 mEq, the
heart restarted with a marked sinus tachycardia.
The cause of hyperhidrosis apparently originates from some poorly understood stimulation of the sympathetic nervous system (Cloward 1969), and in sensitive patients this may possibly lead to excessive vagal stimulation to counteract it, as illustrated by the bradycardia and asystolic reaction to the sudden removal of the sympathetic control, and by the high doses of sympathomimetic drugs necessary to recommence cardiac activity. Anatomically the heart is innervated by the cardiac plexus which consists of the cardiac nerves derived from the cervical and upper thoracic ganglia of the sympathetic trunk and branches of the vagus.The pacemaker of the heart, the sino-atrial node, is innervated by both the parasympathetic and sympathetic nerves (King and Coakley 1958). The ventricular muscle of the heart is supplied solely by the sympathetic nerves, and the larger branches of the coronary arteries are also predominantly innervated by sympathetics (Woollard 1926). These factors may also have a bearing on the hazard of a bilateral cervico- thoracic sympathectomy, which leaves the heart solely under vagal control. Usually, following
denervation, the heart will initiate its own impulse, without recourse to external agencies, but there may be a place for transvenous electrode cardiac pacing, if spontaneous initiationof impulse is delayed, or bradycardia is severe.
R. F. Y. ZEE*
Royal Perth Hospital, Perth
Anaesthesia and Intensive Care, Vol. V, No. 1, February, 1977, Australia
Two episodes of asystolic arrest occurred during the 2nd stage left Cervico-Thoracic sympathec- tomy.
Thirty-five minutes after starting the operation, as the surgeon was retracting and dissecting the upper thoracic chain,
the cardiac monitor showed sudden onset of sinus bradycardia. The pulse rate was 50 beats per minute. Atropine 1·2 mg was given intravenously but cardiac asystole occurred.
External cardiac compression was started and another dose of atropine 1· 2 mg was given, followed by adrenaline 1·0 mg but there was no response. Following a second dose of adrenaline 1·0 mg and sodium bicarbonate 100 mEq, the
heart restarted with a marked sinus tachycardia.
The cause of hyperhidrosis apparently originates from some poorly understood stimulation of the sympathetic nervous system (Cloward 1969), and in sensitive patients this may possibly lead to excessive vagal stimulation to counteract it, as illustrated by the bradycardia and asystolic reaction to the sudden removal of the sympathetic control, and by the high doses of sympathomimetic drugs necessary to recommence cardiac activity. Anatomically the heart is innervated by the cardiac plexus which consists of the cardiac nerves derived from the cervical and upper thoracic ganglia of the sympathetic trunk and branches of the vagus.The pacemaker of the heart, the sino-atrial node, is innervated by both the parasympathetic and sympathetic nerves (King and Coakley 1958). The ventricular muscle of the heart is supplied solely by the sympathetic nerves, and the larger branches of the coronary arteries are also predominantly innervated by sympathetics (Woollard 1926). These factors may also have a bearing on the hazard of a bilateral cervico- thoracic sympathectomy, which leaves the heart solely under vagal control. Usually, following
denervation, the heart will initiate its own impulse, without recourse to external agencies, but there may be a place for transvenous electrode cardiac pacing, if spontaneous initiationof impulse is delayed, or bradycardia is severe.
R. F. Y. ZEE*
Royal Perth Hospital, Perth
Anaesthesia and Intensive Care, Vol. V, No. 1, February, 1977, Australia
Monday, February 6, 2012
A statistically significant drop in the level of norepinephrine occurred in all assessed patients after sympathectomy - the 'lobotomy' effect
http://icvts.oxfordjournals.org/content/5/4/464.full
As a stress hormone, norepinephrine affects parts of the brain where attention and responding actions are controlled.
Along with epinephrine, norepinephrine also underlies the fight-or-flight response, directly increasing heart rate,
triggering the release of glucose from energy stores, and increasing blood flow to skeletal muscle.
Norepinephrine is also released from postganglionic neurons of the sympathetic nervous system, to transmit the
fight-or-flight response in each tissue respectively. The adrenal medulla can also be counted to such postganglionic
nerve cells, although they release norepinephrine into the blood.
Norepinephrine system
The noradrenergic neurons in the brain form a neurotransmitter system, that, when activated, exerts effects on large
areas of the brain. The effects are alertness and arousal, and influences on the reward system.
www.caam.rice.edu/~cox/wrap/norepinephrine.pdf
Thursday, February 2, 2012
"I think the surgeons may not be aware of the long term consequences of denervation"
Email response from Dr. Ahmet Hoke of John Hopkins School of Medicine, School of Neurology - Specifically I asked him his opinion on three things:
1. What was his opinion of ETS in terms of risks vs benefits
2. His opinion on why Thoracic surgeons would advertise a surgical reversal approach when, as he sees it, it would have a very low probability of success
3. His opinion on the Davinci Robot Reversal article regarding surgical reattachment of the sympathetic nerves
1. It all depends on the risk benefit analysis, for some patients yes it may make sense as not everyone develops as severe side effects.
2. I think the surgeons may not be aware of the long term consequences of denervation.
The paper you refer to is not a good model of what happens to the patients because they cut the nerve and immediately repaired it. In such immediate repairs, the ganglia does not loose it's neurons and can regenerate. A better model would be to cut the nerves, wait 6 months and then do the repair; I suspect the recovery would be a lot less.
Ahmet Hoke M.D., Ph.D. FRCPC
Professor of Neurology and Neuroscience
Director, Neuromuscular Division
Johns Hopkins School of Medicine
Department of Neurology
855 N. Wolfe St., Neurology 248
Baltimore, MD, 21205
USA
1. What was his opinion of ETS in terms of risks vs benefits
2. His opinion on why Thoracic surgeons would advertise a surgical reversal approach when, as he sees it, it would have a very low probability of success
3. His opinion on the Davinci Robot Reversal article regarding surgical reattachment of the sympathetic nerves
1. It all depends on the risk benefit analysis, for some patients yes it may make sense as not everyone develops as severe side effects.
2. I think the surgeons may not be aware of the long term consequences of denervation.
The paper you refer to is not a good model of what happens to the patients because they cut the nerve and immediately repaired it. In such immediate repairs, the ganglia does not loose it's neurons and can regenerate. A better model would be to cut the nerves, wait 6 months and then do the repair; I suspect the recovery would be a lot less.
Ahmet Hoke M.D., Ph.D. FRCPC
Professor of Neurology and Neuroscience
Director, Neuromuscular Division
Johns Hopkins School of Medicine
Department of Neurology
855 N. Wolfe St., Neurology 248
Baltimore, MD, 21205
USA
diabetic autonomic neuropathy has already sympathectomized the patient
This diabetic syndrome has been attributed to a lesion of the sympathetic nerve fibres which control sweat secretion [11] and follow the course of the peripheral nerves [12]. This affects the efferent branch of the reflex arch and is identical to that occurring distal to a surgical sympathectomy [13].
There was no difference found between the histological changes in the nerves of the spontaneous anhidrotic patients (Fig. 1) and those of the two previously sympathectomized patients.
A number of papers have been published which stressed [22-24] the high failure rate of sympathectomy operations in diabetics. We believe that the failure of the operation is due to the fact that diabetic autonomic neuropathy has already sympathectomized the patient. The results of the present study are compatible with this idea.
http://www.springerlink.com/content/v21h52461037653k/
There was no difference found between the histological changes in the nerves of the spontaneous anhidrotic patients (Fig. 1) and those of the two previously sympathectomized patients.
A number of papers have been published which stressed [22-24] the high failure rate of sympathectomy operations in diabetics. We believe that the failure of the operation is due to the fact that diabetic autonomic neuropathy has already sympathectomized the patient. The results of the present study are compatible with this idea.
http://www.springerlink.com/content/v21h52461037653k/
Saturday, January 28, 2012
extreme case of compensatory truncal hyperhidrosis and anhidrosis over the head and neck region which led to a heatstroke
Thoracic sympathectomy is a commonly performed surgical procedure for the treatment of palmar hyperhidrosis. However, one major complication of such a procedure is compensatory truncal hyperhidrosis. We describe an extreme case of compensatory truncal hyperhidrosis and anhidrosis over the head and neck region which led to a heatstroke.
http://icvts.oxfordjournals.org/content/early/2011/12/20/icvts.ivr121.abstract?sid=89a2ce71-1ea3-4573-9e63-17329e7c09cd
Sunday, January 15, 2012
PATHOPHYSIOLOGY OF ONE-LUNG VENTILATION
In estimating the degree of shunt that is created by one-lung ventilation when it is performed in the lateral decubitus position, on average, 40% of cardiac output perfuses the nondependent lung and the remaining 60% perfuses the dependent lung (Fig. 1).15 Mechanisms that tend to decrease the percent of cardiac output perfusing the nondependent, nonventilated lung are passive (e.g., mechanical-like gravity, surgical manipulation, amount of pre-existing lung disease) or active (e.g., hypoxic pulmonary vasoconstriction).15 The normal response of the pulmonary vasculature to atelectasis is an increase in pulmonary vascular resistance (in the atelectatic lung), and the increase in atelectatic lung resistance is almost entirely caused by hypoxic pulmonary vasoconstriction. Hypoxic pulmonary vasoconstriction is a protective reflex mechanism that diverts blood flow away from the atelectatic lung. With an intact hypoxic pulmonary vasoconstriction response, the transpulmonary shunt through the nondependent lung decreases to approximately 23% of the cardiac output (see Fig. 1).
Anesthesiology Clinics of North America
Volume 19, Issue 3, 1 September 2001, Pages 435-453
Anesthesiology Clinics of North America
Volume 19, Issue 3, 1 September 2001, Pages 435-453
hypoxic pulmonary vasoconstriction may be impaired after Sympathectomy
It is well known that hypoxic pulmonary vasoconstriction(HPV) plays an important role to protect hypoxemia during the atelectasis induced by one-lung ventilation. Thoracic sympathectomy may have effects on pulmonary vasculature(HPV) and hemodynamics during one-lung anesthesia.
Mean arterial blood pressure was decreased from 81.9+/-2.89 to 73.2+/-2.49 mmHg after thoracic sympathectomy and heart rate was decreased from 104.4+/-3.12 to 88.2+/-2.31beats/min. Arterial oxygen tension was decressed from 570.5+/-17.9 to 521.4+/-23.2mmHg after position change, and decreased to 271.1+/-28.1 mmHg under one-lung ventilation, and finally decreased to 217.0+/-18.3 mmHg after thoracic sympathectomy. With the above results, we can conclude that patients for TES should be carefully observed during and after the procedure, and hypoxic pulmonary vasoconstriction may be impaired after TES.
Korean J Anesthesiol. 1993 Aug;26(4):695-699.
Mean arterial blood pressure was decreased from 81.9+/-2.89 to 73.2+/-2.49 mmHg after thoracic sympathectomy and heart rate was decreased from 104.4+/-3.12 to 88.2+/-2.31beats/min. Arterial oxygen tension was decressed from 570.5+/-17.9 to 521.4+/-23.2mmHg after position change, and decreased to 271.1+/-28.1 mmHg under one-lung ventilation, and finally decreased to 217.0+/-18.3 mmHg after thoracic sympathectomy. With the above results, we can conclude that patients for TES should be carefully observed during and after the procedure, and hypoxic pulmonary vasoconstriction may be impaired after TES.
Korean J Anesthesiol. 1993 Aug;26(4):695-699.
Friday, January 13, 2012
Changes in cerebral morphology consequent to peripheral autonomic denervation
Our findings suggest that peripheral autonomic denervation is associated with grey matter loss in cortical regions encompassing areas that we have previously shown are functionally involved in generation and representation of bodily states of autonomic arousal. The nature of these changes cannot be determined from morphometric analysis alone, but we suggest that they reflect experience-dependent change consequent upon loss of afferent input to brain regions involved in representation of autonomic states.
http://dx.doi.org/doi:10.1016/S1053-8119(03)00011-9
http://dx.doi.org/doi:10.1016/S1053-8119(03)00011-9
Thursday, January 12, 2012
Dopaminergic regulation of cerebral cortical microcirculation
Nature Neuroscience 1, 286 - 289 (1998)
doi:10.1038/1099

doi:10.1038/1099
1 Section of Neurobiology, Yale University School of Medicine, New Haven, Connecticut 06510, USA
2 Department of Psychiatry, Yale University School of Medicine, New Haven, Connecticut 06510, USU
Functional variations in cerebral cortical activity are accompanied by local changes in blood flow, but the mechanisms underlying this physiological coupling are not well understood. Here we report that dopamine, a neurotransmitter normally associated with neuromodulatory actions, may directly affect local cortical blood flow. Using light and electron-microscopic immunocytochemistry, we show that dopaminergic axons innervate the intraparenchymal microvessels. We also provide evidence in an in vitro slice preparation that dopamine produces vasomotor responses in the cortical vasculature. These anatomical and physiological observations reveal a previously unknown source of regulation of the microvasculature by dopamine. The findings may be relevant to the mechanisms underlying changes in blood flow observed in circulatory and neuropsychiatric disorders.Tuesday, January 10, 2012
distinct patterns of peripheral physiological activity are associated with different emotion
The existence of specific somatic states associated with different emotions remains controversial. In this study, we investigated the profile of cardiorespiratory activity during the experience of fear, anger, sadness and happiness. ECG and respiratory activity was recorded in 43 healthy volunteers during the recall and experiential reliving of one or two potent emotional autobiographical episodes and a neutral episode. Univariate statistics indicated that the four emotions differed from each other and from the neutral control condition on several linear and spectral indices of cardiorespiratory activity. Dependent variables were further reduced to five physiologically meaningful factors using an exploratory principal component analysis (PCA). Multivariate analyses of variance and effect size estimates calculated on those factors confirmed the differences between the four emotion conditions. A stepwise discriminant analyses predicting emotions using the PCA factors led to a classification rate of 65.3% for the four emotions (chance=25%; p=0.001) and of 72.0-83.3% for pair-wise discrimination (chance=50%; p's<0.05). These findings may be considered preliminary in view of the small sample on which the multivariate approach has been applied. However, this study emphasizes the need to better characterize the multidimensional factors involved in cardio-respiratory regulation during emotion. These results are consistent with the notion that distinct patterns of peripheral physiological activity are associated with different emotions.
http://www.ncbi.nlm.nih.gov/pubmed/16439033
http://www.ncbi.nlm.nih.gov/pubmed/16439033
Subscribe to:
Posts (Atom)