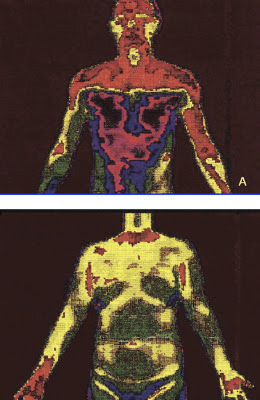
(A) Clear cut change of skin temperature after a T2 sympathicotomy. (B) An even distribution of skin temperature after ramicotomy.
Gossot and colleagues
[8] analyzed a group of T2, T3, T4 sympathectomy
patients in comparison with a group of patients undergoing a
T2, T3, T4 ramicotomy and they reported no statistical difference
regarding the incidence of CS between the two groups studied
(72.2% and 70.9%). However in terms of the severity of CS (embarrassing,
disabling) causing inconveniences to daily life, they reported
27% and 13% incidences in these two groups, respectively. These
findings suggest that by preserving the sympathetic trunk, it
was possible to reduce the severity of CS.
The preganglionic fibers of the sympathetic nerve to the arm
originate mostly from the spinal segments T3–T6 and the
postganglionic fibers of the sympathetic nerve to the arm originate
from T2 and, to a lesser extent, the T3 ganglia
[9]. This implies
that the division of preganglionic fibers (rami communicantes)
reduces the extent of denervation of the sympathetic nerve as
compared with the division of postganglionic fibers (sympathetic
trunk) in the treatment of palmar hyperhidrosis.
Sympathectomy or sympathicotomy is one of the procedures used
to divide the sympathetic trunk. Sympathicotomy distinctively
changes sympathetic nerve distribution in comparison with a
ramicotomy.
Figure 4A illustrates the clear-cut changes of
skin temperature after a T2 sympathicotomy. However the overall
sympathetic nerve distribution to the body is not markedly changed
after a T3 ramicotomy because a T3 ramicotomy is a procedure
that is used to divide one of the preganglionic fibers and to
preserve the sympathetic trunk.
Figure 4B illustrates an even
distribution of skin temperature after T3 ramicotomy.
http://ats.ctsnetjournals.org/cgi/content/full/78/3/1052#FIG4

 http://www.sympatix.fi/blog/?lang=en_
http://www.sympatix.fi/blog/?lang=en_